Monitoring is becoming less dependent on the patient
Continuous monitoring has often depended on charged devices, home hubs and reliable connectivity — a setup that can fail exactly where it is needed. That barrier is beginning to lift. Battery-free body sensors now run on power harvested from a nearby phone or reader,1 and passive backscatter sensors transmit using ambient Wi-Fi rather than their own powered radio.2 The significance is not a better wristband. It is monitoring that asks less of the patient — less charging, less logging, less screen time and fewer setup failures.
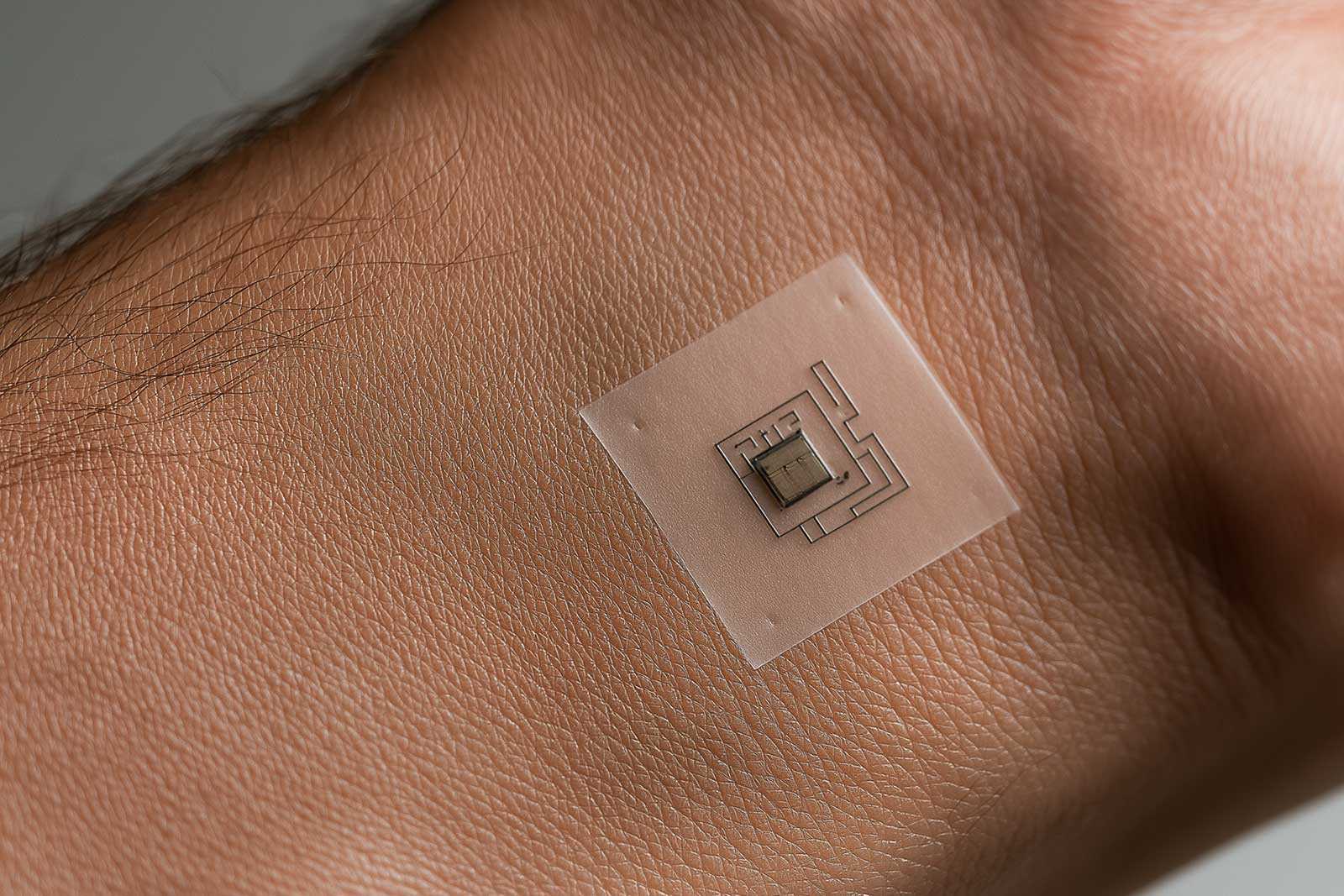
Image · battery-free passive sensing