In 2025, FDA-cleared trials moved pig kidneys beyond one-off exceptions
For years, pig kidney xenotransplants in living patients happened through individual expanded-access cases. In 2025, the FDA cleared investigational clinical trials for gene-edited pig kidneys from United Therapeutics and eGenesis, using source pigs with 10 and 69 gene edits, respectively.1 United Therapeutics’ kidney includes an inactivated porcine gene associated with organ growth, so the transplanted kidney is designed not to keep growing inside a human body. That is more than substitution. It is an early form of biological redesign.

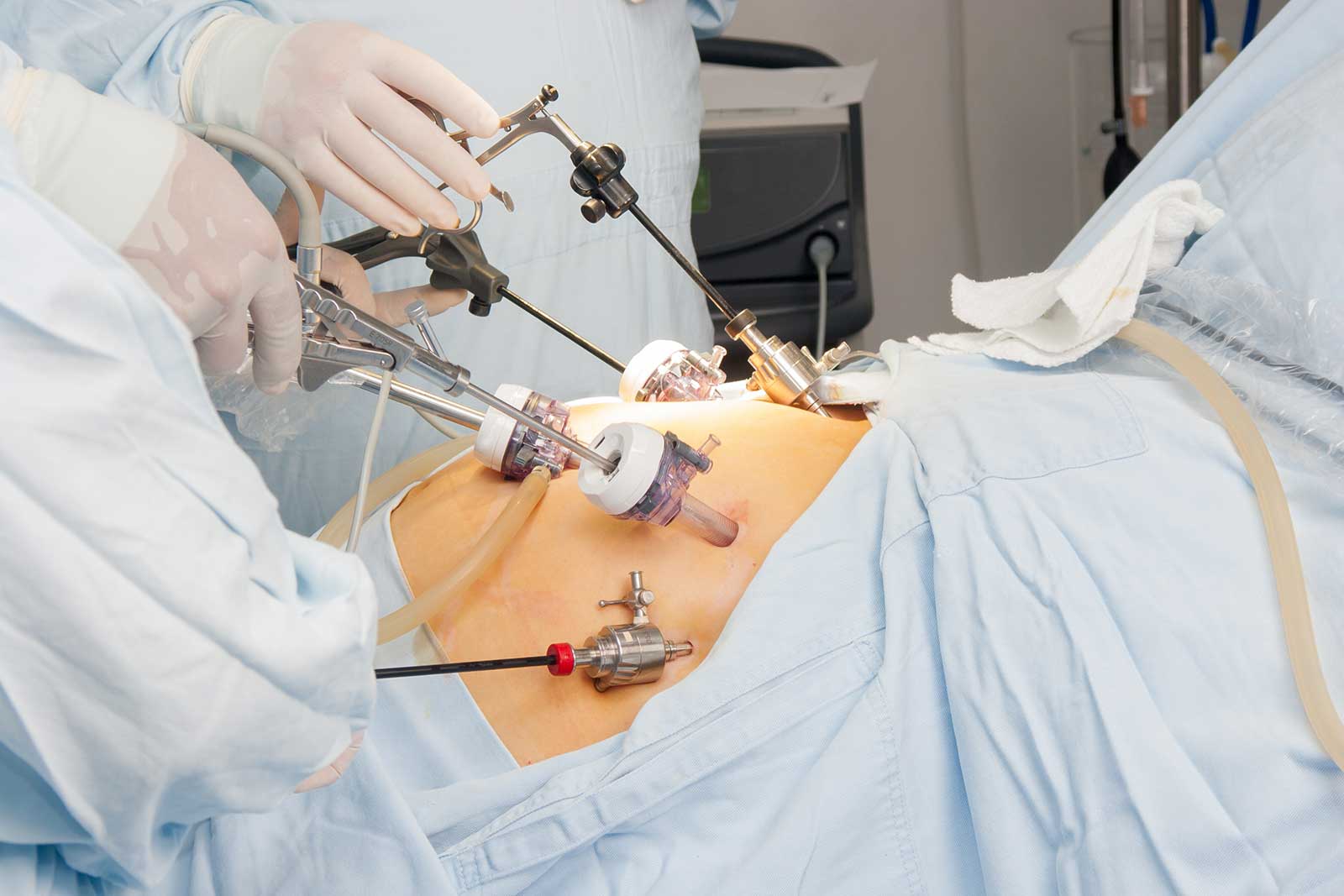
Image · regulated xenotransplant trials