Care delivery redesign + continuous care
Redesigning recovery as a continuous care system.
Most of recovery happens outside the hospital. We redesigned it for the whole journey — including parts the institution doesn’t see.

Most of recovery happens outside the hospital. We redesigned it for the whole journey — including parts the institution doesn’t see.
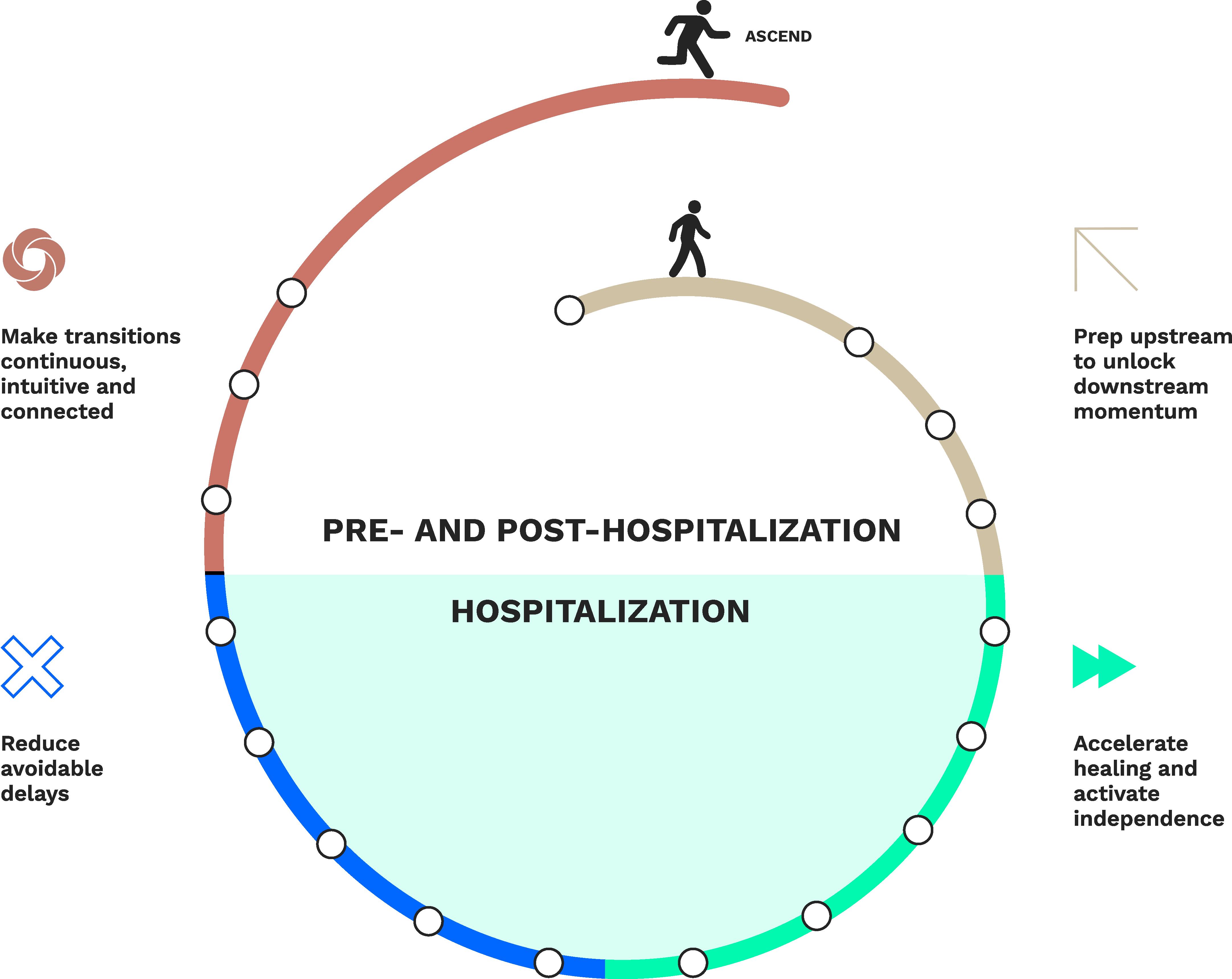
A major academic medical center engaged us to examine the parts of recovery that happen outside the institution’s line of sight — the weeks before admission, the hours after the wristband comes off, the long stretch when the system has mostly stopped checking in.
The work examined what would have to change for these stretches to feel like one connected arc, rather than a series of handoffs patients have to translate between.
Strategic foresight, systems thinking and service design were the tools. But the work kept circling back to a simpler question: what does it actually look like when a system shows up for someone after they’ve gone home?
What happens when healthcare stops thinking in encounters and starts thinking in momentum?
Care still operates through fragmented handoffs between departments, settings, technologies and care teams.
Preparation often begins too late. Coordination depends on manual workarounds — a nurse’s notebook, a forwarded text, a calendar invite no one updated. Patients and families end up inheriting the complexity the system never resolved. And recovery momentum frequently collapses the moment institutional care ends.
Meanwhile, care has moved. Into living rooms, into phones, into the spaces between formal settings. The systems holding it together mostly weren’t built for that.
The work explored what it would take for recovery to stop feeling like a series of recoveries — each one starting over, each one inheriting the residue of the last.
The harder question wasn’t how to improve any single touchpoint. It was how people, technologies and care teams stay aligned on someone’s recovery when no one of them sees the whole picture.
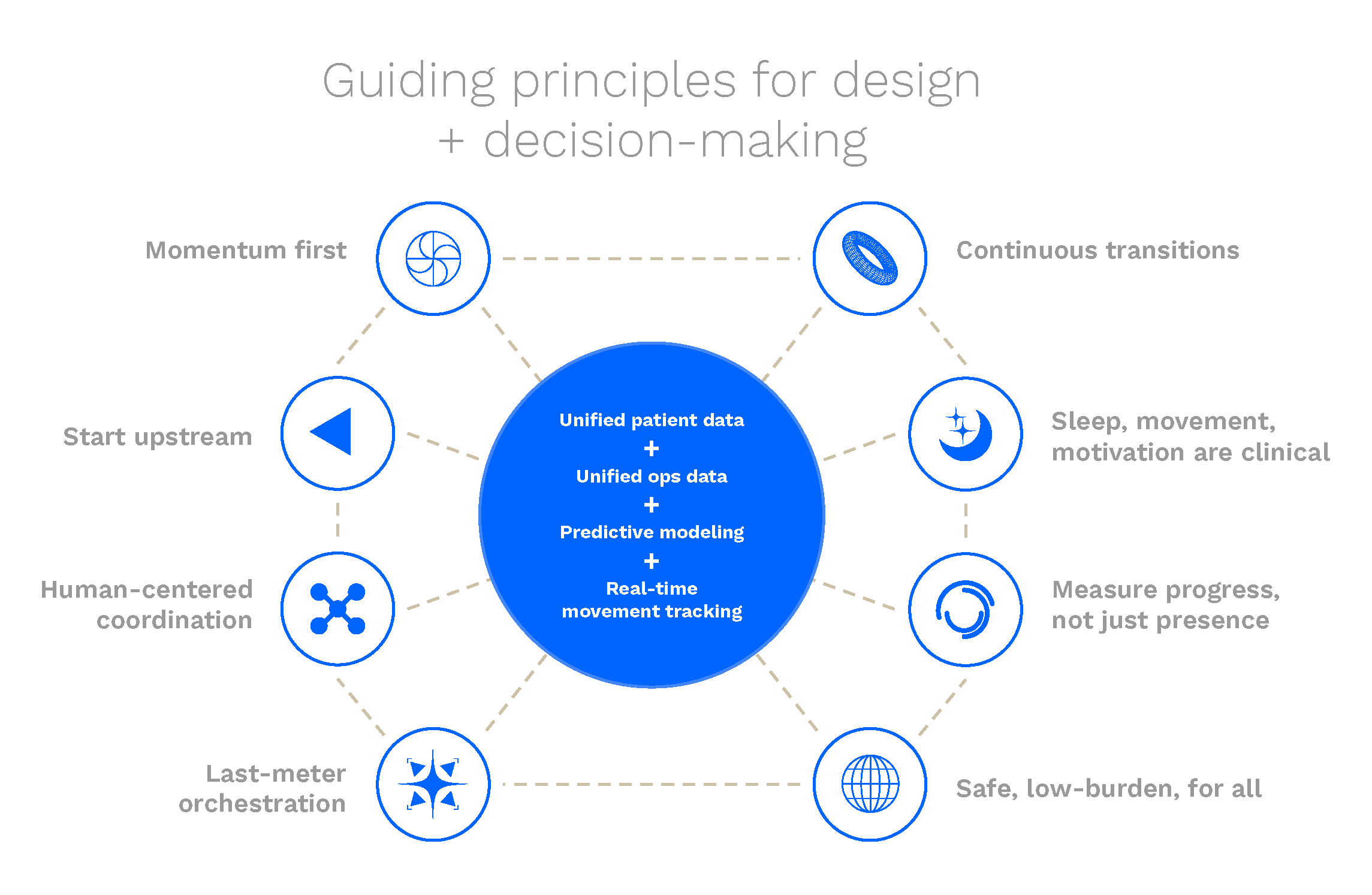
The goal is not adding more visible technology into the care experience.
The goal is reducing friction, uncertainty and fragmentation so patients, caregivers and clinicians can focus more fully on recovery itself.
The strongest systems often become the least noticeable.
The effort helped leadership see what was already happening. Recovery has been moving — into homes, into apps, into the long stretches between formal care. The institutions built to hold it weren’t designed for that movement.
The work reframed the institutional encounter — not as the destination, but as one passage in a longer arc the system rarely sees end-to-end.
The future of recovery may depend less on what happens inside the hospital and more on how seamlessly support continues before and after it.
Start a conversation ↗
Exploring how ambulatory, distributed and longitudinal care models could reshape the future of oncology.
View
Building emotional clarity into the systems, spaces and communications that surround complex care journeys.
View
Rethinking frontline roles, spatial flow and service coordination to reduce friction during high-stress arrivals.
View